Alcohol use disorder can lead to serious insomnia. But treating it is difficult—what’s going on in the brain during this withdrawal-related condition remains largely mysterious.
The Utah MRI Research Center (UMRC) Department of Radiology and Imaging Sciences has completed the installation of Utah's first Siemens Free.Max—an MRI scanner that operates at a field strength of...
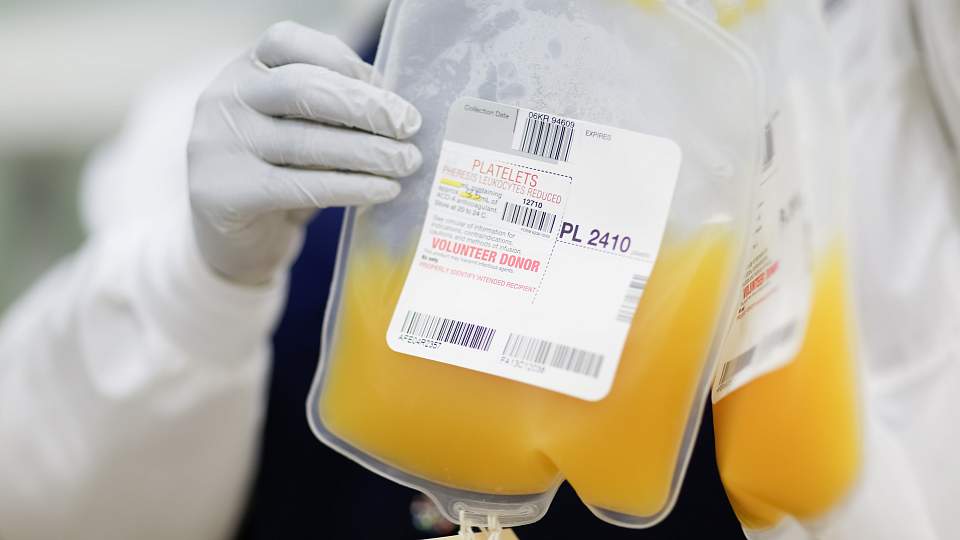
Historic hospital groundbreaking in West Valley City, revolutionary HIV prevention drug receives FDA approval, nursing gerontology program earns five-year accreditation, and more June highlights.
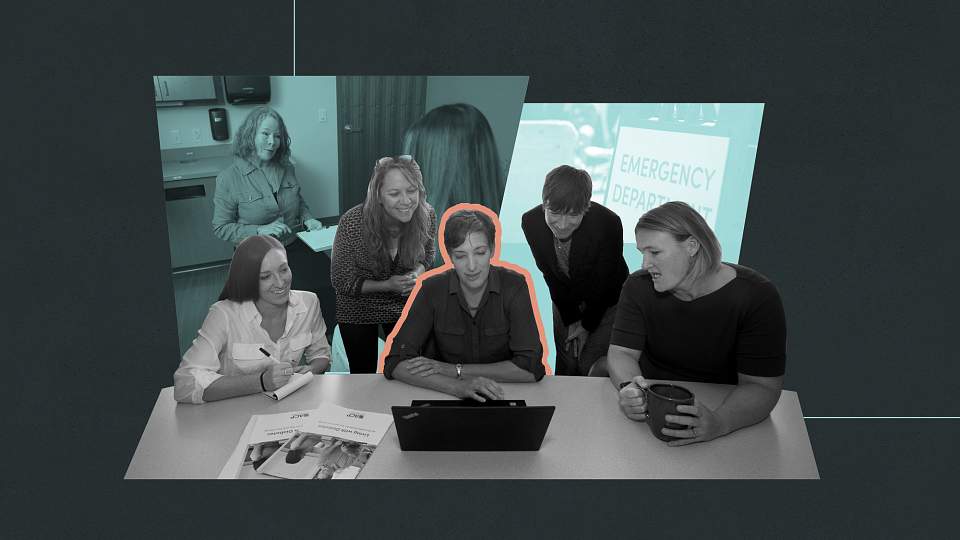
For three decades, the ELAM program has shaped women leaders in academic health. At U of U Health, this commitment reflects our institutional priority to support and elevate women leaders.
Since its beginnings, University of Utah Health has fostered some of the best minds in research. We created genome analysis technologies and now apply them to rapidly diagnose disease in...
Health care professionals are especially prone to stress and burnout. Taking time to be outside—even just for a few minutes—and recreate is key to treating and preventing burnout.
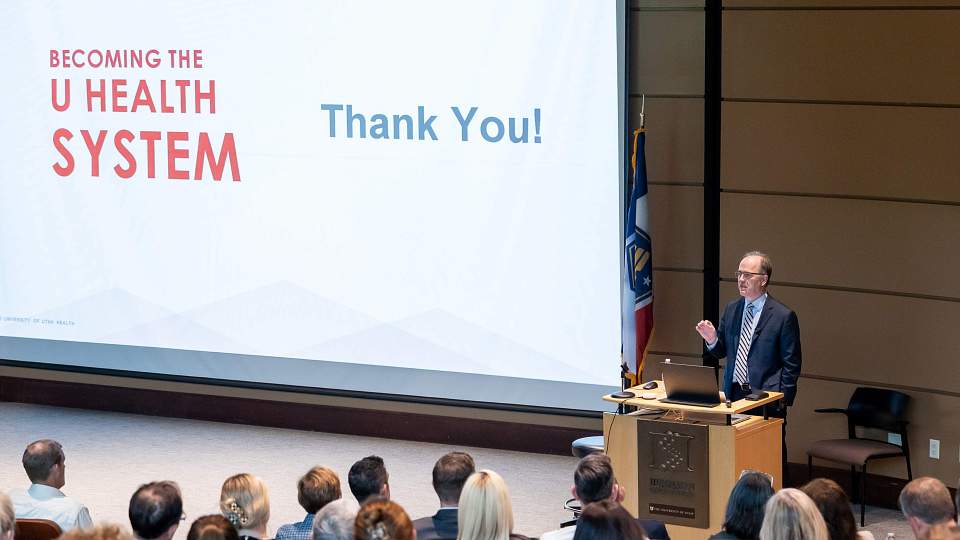
With Utah’s rapid growth reshaping demand for care, U of U Health is evolving from a single-site academic medical center into an interconnected, high-performing health system.
New research shows that weight stigma—and not weight itself—has the biggest impact on mental health and healthy behaviors in the years after weight-loss surgery.
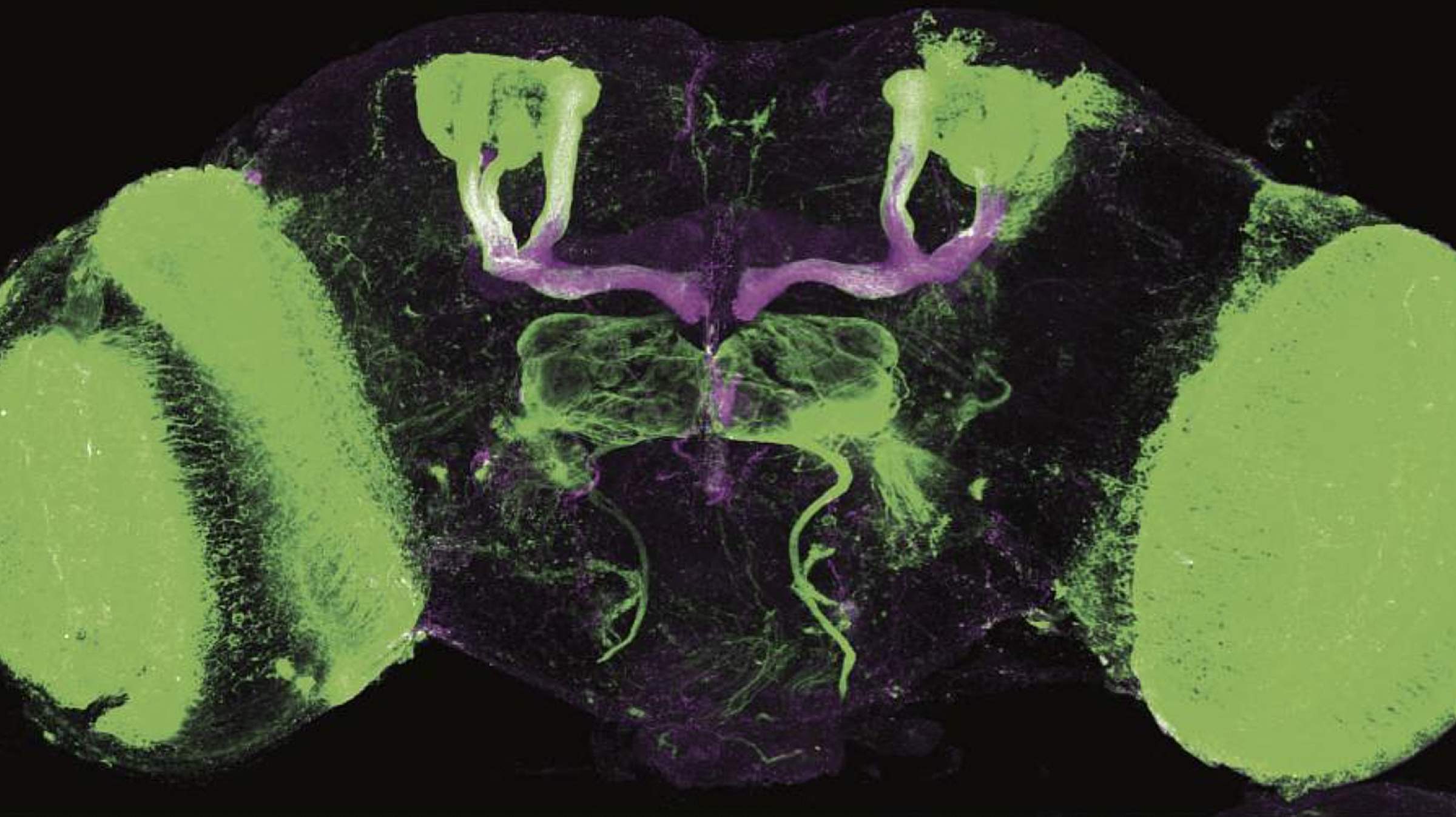
For the first time, researchers have created fruit flies that can become addicted to cocaine. The new model could prove valuable for the development of therapies to prevent and treat...
Top place to work in health care, Moran Eye Center founding CEO retires after 46 years, dental care now covered under Medicaid, new leaders, commencement, and more May momentos.