Voices of U of U Health
Determining High-Risk Individuals for COVID-19
A new front in our fight against COVID-19 is protecting individuals who tend to be at highest risk for requiring hospitalization should they contract coronavirus. We can determine the most vulnerable by looking at data from different groups who live and work in high density environments. By comparing similar groups while factoring in health, fitness, and age, a clear picture emerges of people at highest risk of requiring hospital admission to treat their coronavirus infection.
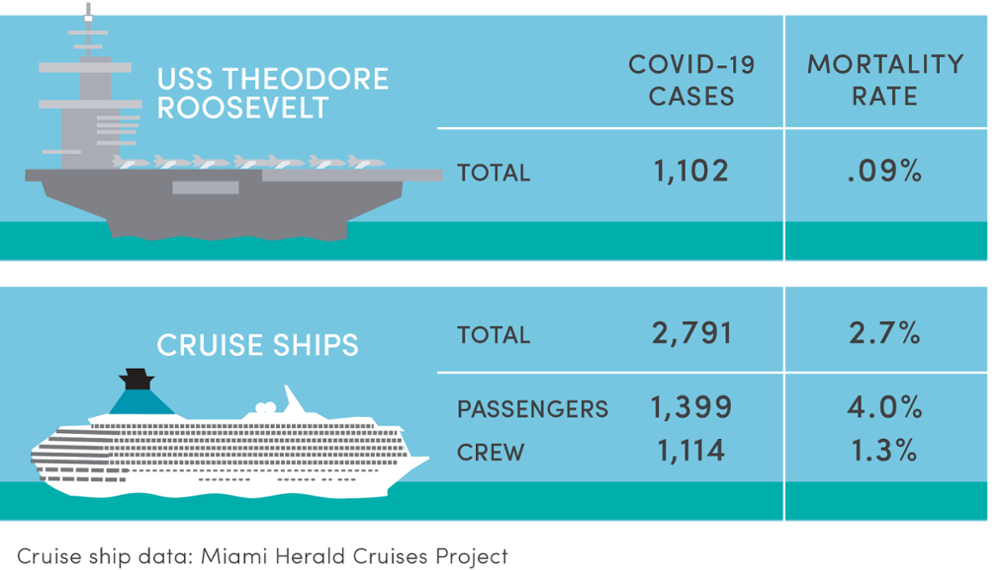
As a comparative example, let’s go out to sea: the USS Theodore Roosevelt is a 1000-foot nuclear-powered aircraft carrier and part of the United States’ Pacific Fleet. Currently it is docked off Guam. As of May 7, the Navy reported there were 1,102 active cases of COVID-19 aboard the ship among a crew of more than 4,000. Coronavirus spreads easily on a vessel because of the high number of sailors on board who are living and working in close confines. Among those contracting COVID-19, there were just seven hospitalized and only one death.
If the number of hospitalizations among active cases seems low, keep in mind the average age of enlisted sailors is 27.3 years. Among officers, the average age is 35.2. Also keep in mind the nation’s armed forces depend on men and women who are fit, healthy, and able to perform at their peak so they do not allow people with certain chronic medical conditions and obesity to join the ranks.
Age and Fitness Factors
Age and level of fitness among US Navy crews is different than among cruise ship passengers, who are generally less healthy due to age alone, and therefore more vulnerable to contracting coronavirus. Typically, among cruise ship passengers, there is a high rate of people living with chronic health conditions. No government or international regulatory agency is comprehensively tracking cases of COVID-19 linked to cruise ships — at least not publicly. The Miami Herald has created the most comprehensive tracking system of coronavirus cases linked to the cruise industry. Its latest update, published May 8, tallies 2,791 cases and 76 deaths. On cruise ships the mortality rate among those infected was 2.7 percent. Aboard the USS Roosevelt, the rate was .09 percent. Passengers on cruise ships were 30 times more likely to die after COVID-19 infection than infected sailors also on a seagoing vessel.
The disparity here between coronavirus outcomes is striking. Similar to older and less healthy people living at high density as those vacationing on cruise ships—and especially those living in nursing home and other long-term care facilities—these populations are at a high risk of being infected and hospitalized, or even dying from the coronavirus, according to the Centers for Disease Control. COVID-19 can spread more easily through high-density facilities, where many people live in a confined environment and workers move from room to room. While just 11% of the country’s cases have occurred in long-term care facilities, deaths related to Covid-19 in these facilities account for more than a third of the country’s pandemic fatalities.
I’m a member of the Medical Advisory Team for the Utah Public Health and Economic Emergency Commission. At our last meeting, we reviewed current CDC guidelines for “People Who Are at Higher Risk for Severe Illness” and concur with the list of medical conditions. Members shared experiences from their health systems, noting obesity, diabetes, pulmonary disease, especially asthma, and hypertension common among patients admitted to their hospitals with COVID-19.
Guidelines for High-Density Living
The Advisory Team also concurred with the CDC notes that high density living environments facilitate virus transmission. These may include nursing homes, assisted living, other long term care facilities; shelters, group homes, and other forms of communal living; multi-generational or multi-family homes; and jails, prisons, and detention centers.
Of nearly 600 individuals admitted to Utah hospitals with COVID-19, we’ve asked the Utah Department of Health to determine three things about each patient: 1) underlying medical conditions on the CDC list, 2) living environment, and 3) working environment. If such data is available or could be collected on all future hospitalizations, then the Medical Advisory Team can review and prioritize the highest risk of intersecting combinations: medical conditions, living environments, and working environments.
These high-risk combinations can lead to highly focused prevention efforts and, if successful, reduce the number of patients admitted to Utah hospitals with COVID-19.